Inside East Africa’s disease highway as cholera cases double across borders
By Aloys Michael, July 18, 2026Every day, thousands of trucks leave Mombasa Port carrying fuel, food, medicines and consumer goods to destinations across East Africa. Their journeys take them through Nairobi, Nakuru, Eldoret, Malaba and Busia before crossing into Uganda and continuing to Kampala, Kigali, Juba and eastern Democratic Republic of Congo (DRC).
The Northern Corridor is one of Africa’s most important trade arteries, linking economies across the East African Community (EAC). Yet health experts warn that the same transport networks powering regional commerce can also accelerate the spread of infectious diseases.
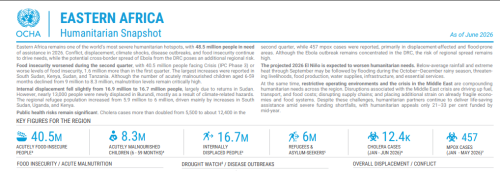
The latest Eastern Africa Humanitarian Snapshot released by the United Nations Office for the Coordination of Humanitarian Affairs (OCHA) highlights the growing challenge. Cholera cases across the region more than doubled during the second quarter of 2026, rising from approximately 5,500 to 12,400 cases, while mpox infections reached 457 cases between January and May. The report notes that many of these outbreaks are occurring in displacement-affected and climate-vulnerable areas.
OCHA warns that conflict, displacement, disease outbreaks and climate shocks continue to compound humanitarian needs across Eastern Africa, which remains “one of the world’s most severe humanitarian hotspots.” An estimated 48.5 million people are expected to require humanitarian assistance in 2026.
The data is raising concerns among public health specialists that East Africa’s increasingly interconnected transport and migration systems could become critical pathways for future disease outbreaks.
Disease routes expand
Public health experts increasingly point to four major drivers behind the growing risk of cross-border disease transmission in East Africa: expanding regional trade, rising population displacement, climate-related disasters and underfunded disease surveillance systems.
The Northern Corridor illustrates how quickly pathogens can move between countries. A truck driver departing Mombasa may interact with hundreds of people before reaching Kampala, including customs officials, traders, transport workers, hotel operators, market vendors and passengers at roadside stops.
The region’s extensive bus networks create similar connections. Thousands of passengers travel daily between Mombasa, Nairobi, Kisumu, Kampala, Kigali and Juba, linking urban centres and border communities through constant human movement.
While trade itself is not the cause of disease outbreaks, increased mobility creates opportunities for infections to spread when surveillance systems, sanitation infrastructure and public health services fail to keep pace.
This is particularly true for cholera, a waterborne disease that thrives in areas with inadequate access to safe water and sanitation. Flooding, overcrowded settlements and weak public-health infrastructure can rapidly increase transmission risks.

Border risks intensify
Conflict and displacement are adding new pressures to regional health systems.
According to OCHA, Eastern Africa hosts approximately 6 million refugees and asylum seekers, alongside 16.7 million internally displaced people. Many travel through border towns, transit centres and informal migration routes before reaching refugee settlements or urban centres.
Key border points such as Malaba, Busia, Namanga and Elegu have become vital economic gateways but also important public-health monitoring locations.
The report notes that mpox cases were reported primarily in displacement-affected and flood-prone areas, highlighting the growing intersection between humanitarian crises and disease outbreaks.
Meanwhile, outbreaks in one country increasingly carry regional implications. OCHA warns that although Ebola remains concentrated in parts of the Democratic Republic of Congo, cross-border population movements continue to elevate the risk of wider transmission.
For countries linked by trade, migration and shared transport infrastructure, disease outbreaks are no longer purely national emergencies.
Health security matters
The rise in cholera cases and continued spread of mpox are reinforcing calls for stronger regional disease surveillance and epidemic preparedness.
Governments across the EAC, IGAD and international health agencies are increasingly investing in border health security, including disease screening, laboratory networks, emergency response systems and real-time outbreak monitoring.
Climate change is adding urgency to these efforts. OCHA warns that below-average rainfall and extreme heat expected through September could be followed by flooding during the October-to-December rainy season. Such conditions can contaminate water sources, damage sanitation infrastructure and increase the likelihood of cholera outbreaks.
The challenge facing East Africa is not how to limit trade, migration or regional integration. Rather, it is how to ensure that public-health systems evolve as rapidly as the movement of people and goods.
As transport corridors become more connected and climate shocks become more frequent, epidemic preparedness will increasingly determine the region’s resilience. The same roads, ports and border crossings that drive economic growth must also become the front lines of disease surveillance.
For East Africa, protecting trade routes may increasingly depend on protecting public health.